We are currently experiencing technical issues with our phone system.For immediate assistance, please email us at contact@belaydiagnostics.com. We apologize for the inconvenience.
Clinical Utility of Belay Summit™ Cerebrospinal Fluid Test to Inform Diagnosis and Management of Central Nervous System Cancer—A Single Institution Case Series
Authors:
Michael Youssef, Alexandra Larson, Vindhya Udhane, Zhixin Jiang, Daniel Lim, Jennifer N. Adams, Rakshitha Jagadish, Anthony Acevedo, Brett A. Domagala, Samantha A. Vo, Tarin Peltier, Daniel Sanchez, Viriya Keo, Julianna Ernst, Kala F. Schilter, Qian Nie and Honey V. Reddi
Detecting central nervous system (CNS) cancers from evaluation of cells in cerebrospinal fluid (CSF) has very low positivity rates, limiting downstream management of these cancers. The Belay Summit CSF-based test has been shown to accurately indicate the presence of cancer in 90% of cases. This study presents the results from a single institution using the Belay Summit liquid biopsy test showing higher sensitivity over CSF cytology testing, providing clinically meaningful information to support physician decision-making for the diagnosis and management of CNS cancers.
Abstract:
Background
Cytology from cerebrospinal fluid (CSF) is standard-of-care to detect central nervous system (CNS) cancers but suffers from low-sensitivity and lacks associated molecular information, often requiring brain biopsy or resection to obtain. Belay Diagnostics offers analytically and clinically validated CSF-based tests to support the diagnosis and management of primary and secondary CNS cancers. However, the clinical utility (CU) of these assays has not been previously evaluated.
Methods
This retrospective study presents a real-world, single institution experience of using the Belay Summit liquid biopsy test for all orders received (n = 123) between October 2024 and September 2025. Clinical information was reviewed for demographics, provisional diagnosis, oncology history, CSF cytology results, and tumor genomic profiling results. The primary endpoint of this study was to evaluate the impact of Belay CSF-based assays on physician diagnosis and treatment decisions. Secondary endpoints included evaluating the clinical performance of the Belay Summit test verses cytology in CNS malignancy detection (sensitivity, specificity, and accuracy).
Results
The cohort included 120 patients with suspected or previously diagnosed primary (n = 40) or metastatic (n = 80) CNS tumors; three patients completed longitudinal testing for a total of 123 specimens and test orders. Summit showed higher sensitivity for CNS malignancy (90%) over CSF cytology (12%). The Belay CSF liquid biopsy test demonstrated strong clinical utility and was essential to clinical course pursued in 93% (114/123) of specimens, informing treatment and management decisions.
Conclusions
The Belay Summit test provides clinically meaningful information to support physician decision-making for the diagnosis and management of primary and secondary CNS tumors, especially in cases where tissue sampling is infeasible.
Figure 1: Overview of Summit results for 123 cerebrospinal fluid (CSF) specimens.
A: Summit detected a clinically significant variant in 62% of specimens (yellow); 38% of samples were negative for clinically significant variants (navy blue).
B. Distribution of positive and negative Summit results in suspected primary or metastatic central nervous system (CNS) disease of varying tissues of origin.
C. Clinically actionable single nucleotide variants (SNV) were detected with or without chromosomal arm-level aneuploidy and MGMT promoter methylation in suspected primary and metastatic CNS specimens.
Figure 2: Summit demonstrated higher sensitivity compared to cerebrospinal fluid (CSF) cytology, with sensitivity not impacted by DNA input. The majority of suspected primary and metastatic tumors had negative CSF cytology results at the time of Belay testing.
A, B. Summit demonstrated higher sensitivity compared to cerebrospinal fluid (CSF) cytology (A), which was not impacted by DNA input (B). Red boxes indicate false negative specimens and the green box indicates the false positive specimen.
C, D. The majority of suspected primary and metastatic tumors had negative CSF cytology results at the time of Belay testing.
E. Summit positivity in primary central nervous system (CNS) tumors in the context of biopsy prior to Belay test. Not otherwise specified, NOS.
F. Summit positivity in metastatic CNS tumors in the context of clinical suspicion of LMD or suspected brain metastasis. Leptomeningeal disease, LMD; metastasis, mets.
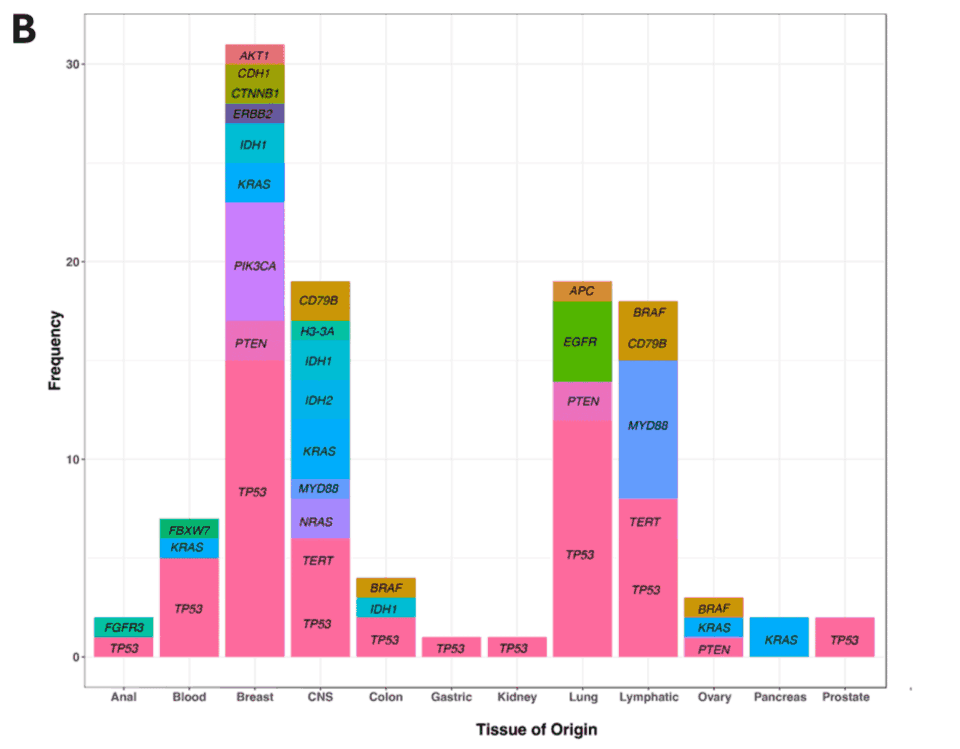
Figure 3: Summary of Summit results for 123 cerebrospinal fluid (CSF) samples.
A. Summit detected gene-level variants and chromosomal arm-level alterations. SNV, single nucleotide variant; INDEL, insertion/deletion; central nervous system, CNS.
B. Clinically significant variants were detected in 21 of the 32 genes included on the Summit panel with different frequencies between tissues of origin.
Figure 4: Variant allelic frequency (VAF) can be used as a quantifiable measure to inform diagnosis of leptomeningeal disease (LMD) and track disease progression and/or response to therapy.
A. VAF greater than 5% reliably informed diagnosis of LMD. Red squares indicate orders with initial concern for (c/f) parenchymal metastasis (mets) and/or leptomeningeal involvement that were confirmed to have LMD upon neuroimaging/clinical presentation after Belay testing, correlating with VAF of detected variants. Central nervous system, CNS.
B, C. VAF of clinically significant variants detected in two longitudinally collected specimens was used to monitor disease progression and therapeutic response (B) or resistance (C).
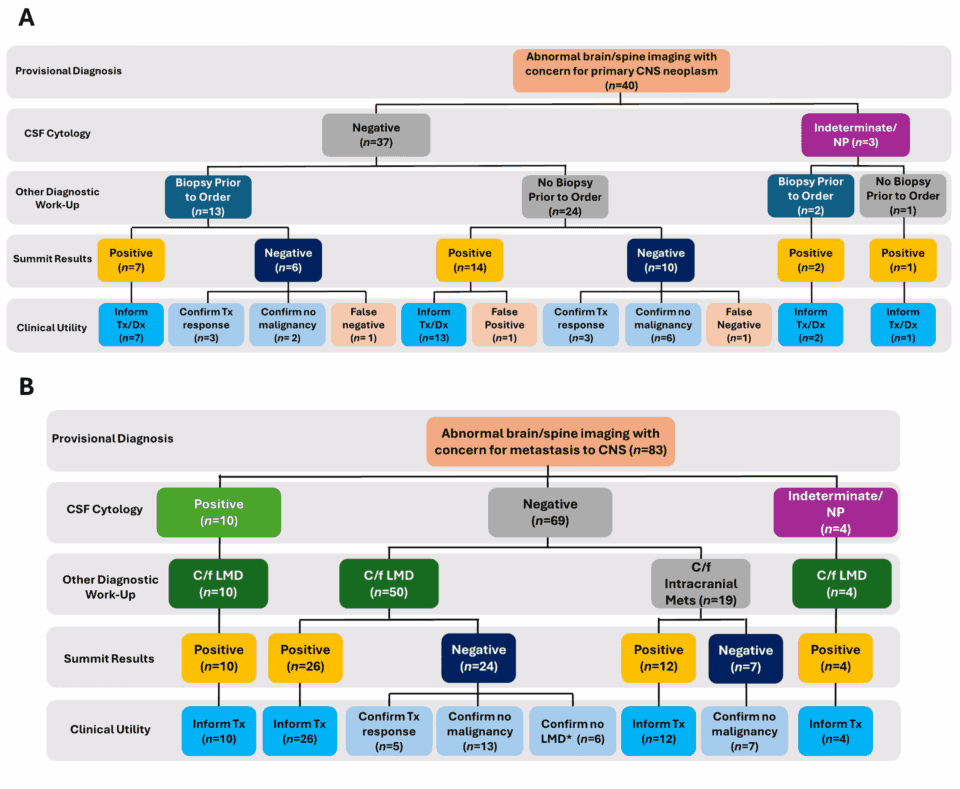
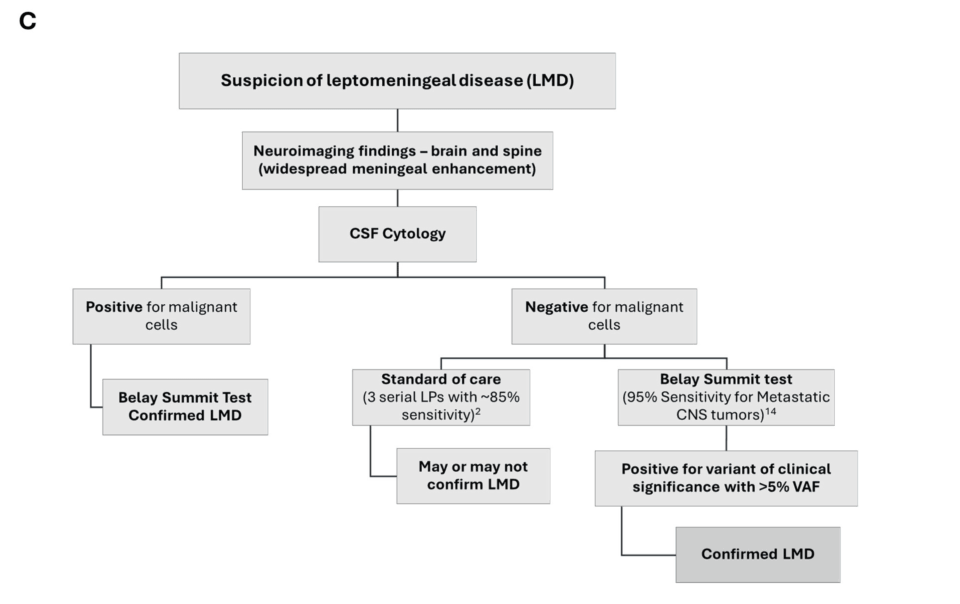
Figure 5: Summit impacts treatment and management of primary and secondary central nervous system (CNS) malignancies.
A, B. Graphical representation of the clinical utility (CU) of Summit alongside cerebrospinal fluid (CSF) cytology following a provisional diagnosis of primary (A) or metastatic (B) CNS disease for 123 samples. Not performed, NP; treatment, Tx; diagnosis, Dx.
C. Schematic of testing algorithm implemented at University of Texas, Southwestern to inform diagnosis of leptomeningeal disease (LMD). Lumbar puncture, LP; variant allelic frequency, VAF.
D. Breakdown of Summit CU impact among 123 samples.